
Your Thyroid Before Pregnancy – Why Your Lab Report May Be Misleading You
I want you to picture something. You have just picked up your blood test report. You scan across the page, find your TSH value, and check it against the reference range printed next to it. Your number falls within the range. The word next to it says ‘Normal’.
You breathe a sigh of relief. Your thyroid is fine.
Except, and this is the part nobody explains, the reference range on that report was not designed with you in mind. Not you as someone planning a pregnancy. Not you as someone whose thyroid is about to be asked to do something it has never had to do before. That range was designed for a non-pregnant adult going about their daily life.
For that purpose, it is perfectly valid. For your purpose of getting pregnant and growing a baby it is the wrong benchmark entirely.
This is a conversation I have in my clinic almost every week. And it is the conversation I want to have with you here, because understanding thyroid before pregnancy India is essential for women who are planning to conceive and want the healthiest possible start to pregnancy.
What TSH Is and What It Is Actually Measuring
Checking TSH before pregnancy is an important part of preconception planning because pregnancy places additional demands on the thyroid gland.
TSH stands for Thyroid Stimulating Hormone. It is produced by the pituitary gland, a small gland at the base of your brain, and its job is to tell the thyroid gland how much hormone to produce. When thyroid output is low, the pituitary responds by producing more TSH, essentially sending a louder signal. When thyroid output is adequate, TSH stays low.
This means TSH works inversely to thyroid function. A high TSH is a sign that the pituitary is working harder than it should because the thyroid is underperforming. A TSH within the normal range means the pituitary is satisfied with what the thyroid is producing.
The question, when you are planning a pregnancy, is whether ‘satisfied’ is good enough. And my answer based on both the evidence and on years of watching what happens when we optimise thyroid function before conception rather than after is that ‘satisfied’ is not the same as ‘optimal’. This is why many women search for TSH 2.5 pregnancy India, as pregnancy planning often requires different thyroid targets than those used for the general adult population.
The Context That Changes Everything
Let me be very clear about something, because I think clarity here is important.
If you came to me with a TSH of 4.2 and you were not planning a pregnancy, had no symptoms, were feeling well, and were living your life normally. I would not treat you. If your TSH were 5, or even 6, and you had no symptoms, I would monitor you and counsel you about what the numbers mean, but I would not reach for a prescription. Subclinical hypothyroidism in a non-pregnant, asymptomatic person is a conversation about monitoring, not necessarily about medication. However, subclinical hypothyroidism preconception deserves closer attention because thyroid function can affect conception and early pregnancy outcomes.
The moment you tell me you are planning a pregnancy, that conversation changes completely. This is one of the key reasons why preconceptional counselling in Kolkata is recommended for couples planning a pregnancy, as it allows thyroid function and other health factors to be evaluated before conception. This is why the relationship between hypothyroidism fertility India is an important consideration during fertility evaluation and treatment. The TSH that was acceptable yesterday becomes clinically significant today. Not because the number changed. Because the context changed.
Your lab report is not wrong. It is simply answering a different question from the one you need answered when you are trying to conceive.
The question you need answered is not ‘Is my thyroid functioning adequately for my current life? The question is, is my thyroid ready for conception, early implantation, and the extraordinary demand of the first trimester of pregnancy? A thyroid test before trying to conceive can help identify thyroid disorders early and ensure appropriate treatment before pregnancy ( tests before pregnancy ) begins. Those are not the same questions. This distinction is central to understanding thyroid before pregnancy India, where pregnancy planning requires thyroid assessment based on conception-specific goals rather than standard laboratory reference ranges.
The Two Reasons I Optimise Thyroid Before Conception – Not After
There are two distinct clinical arguments for getting TSH into the preconception target range before you start trying. Both matter. I want to explain each one clearly.
Reason One – Conception Itself
Thyroid hormones are deeply involved in the female reproductive cycle. They influence the development of the follicle carrying the egg, the quality of the egg within it, the function of the corpus luteum after ovulation, which maintains the early pregnancy by producing progesterone, and the receptivity of the uterine lining to implantation.
Women with subclinical hypothyroidism and a TSH above the preconception target range25 have measurably lower rates of natural conception, higher rates of implantation failure, and higher rates of early pregnancy loss. This is not a theoretical risk. It is a documented clinical pattern.
Correcting thyroid function before the first attempt at conception means the entire process – ovulation, fertilisation, implantation, and early pregnancy maintenance – happens in a body where thyroid hormones are already at the level they need to be. Correcting it after a positive pregnancy test means playing catch-up during a window you cannot get back.
Reason Two – Your Baby’s Brain
This is the reason that, in my experience, changes how couples think about this test. Because it is about something much bigger than getting pregnant. It is about the child you are going to have.
Here is a fact that most people have never been told: in the first ten to thirteen weeks of pregnancy, your baby has no thyroid gland of its own. None. The foetal thyroid does not begin producing hormones until the second trimester. Until that point, every molecule of thyroid hormone that reaches your baby’s developing brain comes entirely from you.
And thyroid hormone, during this window, is not optional for brain development. It is essential. It drives neuronal migration the process by which brain cells travel to their correct locations. It drives the development of the connections between those cells. It drives early myelination the insulation of nerve fibres that allows signals to travel efficiently. These are not processes that can be repeated or corrected later. They happen once, in that first trimester, and the thyroid hormone environment in which they happen matters.
A woman whose TSH was sitting above the preconception target when she conceived, and who only gets tested and started on treatment at eight or ten weeks of pregnancy, has already allowed that first trimester window to partially pass with suboptimal thyroid levels. The baby’s brain was developing in that time. We cannot go back.
Optimising thyroid function before conception means that from the moment of fertilisation from the very first days of that embryo’s existence, the hormonal environment it is developing in is already correct. That is the argument for preconception thyroid optimisation that I find most compelling. And it is the one I think every couple planning a pregnancy deserves to hear.
What the Right TSH Target Is Before Pregnancy
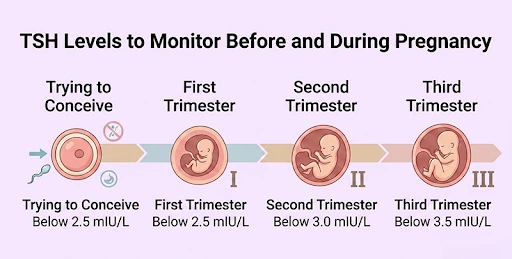
The preconception TSH target I use in my clinical practice is between 2.5 and 3.5 mIU/L. Not below 2.5 that would be overcorrecting into a range that carries its own risks, including suppression of TSH when thyroid hormone levels are too high. Not above 3.5 because that is the zone where the evidence for preconception benefit becomes meaningful.
I want to acknowledge something honestly here: the evidence on exactly where the cutoff should sit has been debated in the medical literature, and guidelines have evolved over time. The American Thyroid Association moved away from a fixed 2.5 cutoff in 2017, acknowledging that population-specific reference ranges matter. In India specifically, some studies suggest that the upper limit of normal TSH in a healthy Indian population may be slightly higher than Western reference ranges.
What this means practically is that I do not treat a number in isolation. I treat a person in a context. A TSH of 3.8 in a woman planning pregnancy with no thyroid antibodies, a family history that is clear, and a previous pregnancy that went smoothly is a different clinical picture from a TSH of 3.8 in a woman with elevated anti-TPO antibodies, a history of miscarriage, and irregular cycles. The number is the starting point. The clinical picture is what guides the decision.
What I can say with confidence is this: if your TSH is above 3.5 and you are planning a pregnancy, that is a conversation worth having with your doctor now, before you start trying. Not after a positive test. Not after a loss. Now.
What Happens If Your TSH Is Outside the Preconception Range
The good news, and it is genuinely good news, is that this is one of the most straightforward things we treat in preconception medicine. Levothyroxine, a synthetic thyroid hormone, is safe, effective, well-tolerated, and has decades of evidence behind it. It is taken once daily, usually in the morning on an empty stomach. The dose is adjusted based on your TSH response. In most cases, TSH can be brought into the target range within four to eight weeks of starting the correct dose.
This is not a medication you take forever necessarily, though many women with true hypothyroidism do need it long-term. In the preconception context, the goal is to get your TSH into the target range before you start trying, maintain it through early pregnancy when foetal brain development depends on it, and then reassess as pregnancy progresses and the dose requirements change.
It is also important to check thyroid antibodies, specifically anti-TPO antibodies, alongside TSH. Women who are antibody positive are at higher risk of thyroid function declining further during pregnancy, even if their TSH is currently within range. Knowing this before conception allows us to monitor more closely and adjust treatment earlier if needed.
The Test Is Simple. The Consequences of Missing It Are Not.
A TSH test costs very little. It is a single blood draw. The result is available within a day or two. And yet it is among the most consequential tests in a preconception panel because what it finds, when it finds something, is both important and entirely correctable.
The couples who benefit most from preconception thyroid testing are not the ones with obvious symptoms fatigue, weight gain, hair loss, and feeling cold all the time. Those women often already know something is off. The couples who benefit most are the ones who feel completely fine, assume their thyroid is normal, and have never had it specifically checked in the context of conception. Maintaining healthy thyroid hormone levels is also essential for thyroid and baby brain development, particularly during the first trimester when the baby depends on the mother’s thyroid hormones.
A normal feeling is not a normal TSH. The only way to know is to test.
Get it checked. Get it into the right range. And then start trying with the confidence that one of the most important hormonal systems in early pregnancy is already working in your favour.
Frequently Asked Questions
My TSH is 3.9, and my doctor says it is normal. Should I be concerned?
Your doctor is not wrong, 3.9 falls within the standard reference range for a non-pregnant adult. But if you are planning a pregnancy, it is worth a specific conversation about preconception thyroid targets. The reference range on your report and the preconception target range are different things, set for different purposes. Bring your report to your preconception consultation, and we will assess it in full context, including antibody status, symptoms, and your reproductive history.
I have been on levothyroxine for years. Do I need to do anything different before trying to conceive?
Yes. Women who are already on levothyroxine often need their dose increased in early pregnancy because the thyroid demand rises significantly. The time to review your dose and get your TSH into the preconception target range is before you start trying, not after a positive test. Bring your most recent thyroid function results to your preconception consultation, and we will assess whether your current dose is adequate for conception.
Can thyroid problems cause miscarriage?
Yes, this is one of the clearest links in preconception thyroid medication. Both overt and subclinical hypothyroidism are associated with higher rates of early pregnancy loss. Thyroid antibodies, even in women whose TSH is within the normal range – are independently associated with increased miscarriage risk. This is why thyroid function is not just a fertility test. It is a pregnancy health test that should be done before the pregnancy begins.
If I start levothyroxine before pregnancy, will I need it for the rest of my life?
Not necessarily. Some women started on levothyroxine for preconception optimisation, who had borderline-high TSH without true autoimmune hypothyroidism, are able to reduce or discontinue the medication after pregnancy. Others, particularly those with anti-TPO antibodies or a TSH that was significantly elevated, may need to continue. This is assessed after delivery, once the post-pregnancy thyroid recovery period has passed. The decision is always made based on how your thyroid is functioning at that point, not on a blanket rule.
Does the husband’s thyroid matter for fertility?
Less directly than the wife’s, thyroid function in men does influence testosterone levels, sperm quality, and overall metabolic health. If a husband has known thyroid disease or symptoms suggestive of thyroid dysfunction, it is worth testing. In the absence of symptoms or history, routine thyroid testing in men before conception is not a universal recommendation, though it may be done based on individual clinical assessment.
Your thyroid report says normal. Let us check if it is optimal.
A preconception thyroid assessment at Renew Healthcare looks at your TSH in the context of conception and early pregnancy – not just routine health. We check antibody status, review your clinical picture, and make a plan that gives your thyroid the best possible chance of supporting both conception and your baby’s developing brain. Book your consultation before you start trying.
WhatsApp / Call: +91 62922 69060
Download your free Zero Trimester Guide: drrajeevagarwal.co.in/preconception/
– Dr. Rajeev Agarwal | Fertility Specialist & Gynaecologist, Renew Healthcare, Kolkata
Don’t just conceive, preconceive. – Dr. Rajeev Agarwal
Popular Services
Vaginismus Therapy In Kolkata | Urinary Laser Therapy In Kolkata | Laparoscopic Surgery In Kolkata | Hysteroscopic Procedure In Kolkata | IVF Specialist In Kolkata
Popular Blogs
Understanding The Role Of Genetics In Ivf Success | Battling Blood Sugar During Pregnancy | How Sleep Affects Hormonal Balance & Fertility In Women | Birth Control Pills For Pcos: How Long Should You Stay On Them? | Can Ovarian Stimulation Affect Your Next Period Cycle?